Question Of the Day
Case: A 14-hour old male newborn baby was delivered at term, he was noted to be jaundiced. He is the first baby in the family. His blood group was A-ve, his mother blood group was O+ve, his Hb was 14gm/di, serum bilirubin was 7 mg/dl, direct Coombs test was +ve.
Question: The most likely diagnosis is:
Correct Answer:
D. ABO blood group incompatibility
This baby has Early-onset jaundice (within 24 hours) → suggests pathological jaundice with blood group incompatibility → baby is A-negative, mother is O-positive. ABO incompatibility is common when the mother is O and the baby is A or B.also Positive direct Coombs test → Indicates immune-mediated hemolysis (maternal antibodies attacking fetal RBCs).with low Hemoglobin 14 g/dL indicates ABO blood group incompatibility.
Why the other options are incorrect:
-
A. Physiological jaundice:
Typically appears after 24 hours, peaks at day 3-5, and resolves without intervention. Jaundice at 14 hours is too early for physiological jaundice. -
B. Breast milk jaundice:
Appears after the first week of life, typically between days 5-7, and persists for weeks. Not relevant in the first 14 hours. -
C. Breastfeeding jaundice:
Associated with insufficient intake in the first few days, leading to dehydration and increased enterohepatic circulation. It’s not usually associated with Coombs-positive hemolysis or this early onset. -
E. Rh blood group incompatibility:
Would be considered if the mother was Rh-negative and the baby was Rh-positive. In this case, the mother is Rh-positive (O+), and the baby is Rh-negative (A−), so Rh incompatibility is not possible.
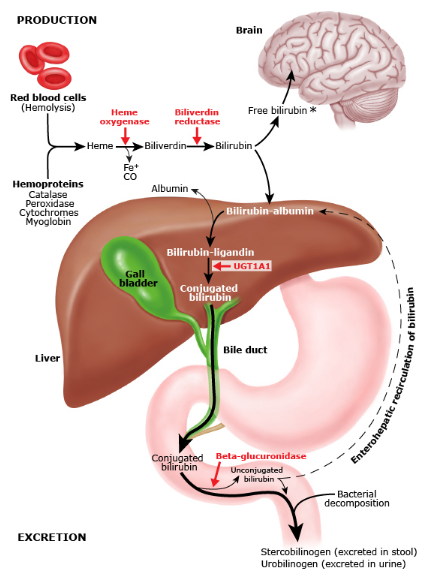
Bilirubin production, metabolism, and excretion
Bilirubin is primarily derived from the breakdown of heme, Heme is broken down by heme oxygenase into biliverdin, which is then converted to unconjugated bilirubin by biliverdin reductase, Unconjugated bilirubin is lipophilic and binds to albumin for transport in the plasma to the liver.In the liver,It undergoes conjugation by UDP-glucuronosyltransferase to form water-soluble conjugated bilirubin. then it is secreted with bile into the small intestine.In the intestine, gut bacteria deconjugate bilirubin and convert it into urobilinogen.Some urobilinogen is reabsorbed and either excreted in urine (as urobilin) or returned to the liver via enterohepatic circulation.The rest is oxidized to stercobilin, which gives stool its brown color.
| Physiological v.s Pathological Jaundice |
||
|---|---|---|
| Feature | Physiological Jaundice | Pathological Jaundice |
| Onset | After 24 hours of birth (usually 2–3 days) | Within 24 hours of birth |
| Peak bilirubin level | <12 mg/dL in term neonates, <15 mg/dL in preterm | >12–15 mg/dL or rapidly rising (>5 mg/dL/day) |
| Cause | Immature liver, increased RBC breakdown, low UGT activity | Hemolysis (ABO/Rh incompatibility, G6PD deficiency), infections, metabolic disorders, biliary atresia |
| Duration | Resolves by 1–2 weeks (term) or 2–3 weeks (preterm) | Persists >2 weeks (term) or >3 weeks (preterm) |
| Type of bilirubin | Unconjugated (indirect) | Mostly unconjugated, but can be conjugated (liver disease, obstruction) |
| Treatment | None usually needed; resolves spontaneously | Requires phototherapy, exchange transfusion, or treating the underlying cause |
| Complications | None | Risk of kernicterus (bilirubin encephalopathy) if untreated |
| Pathological Jaundice |
|||||
|---|---|---|---|---|---|
| Type | Cause | Bilirubin Type | Onset | Key Features | Management |
| Hemolytic Disease of the Newborn (HDN) | ABO or Rh incompatibility | Unconjugated | Within 24 hours | Positive Coombs test, anemia, hepatosplenomegaly | Phototherapy, exchange transfusion |
| G6PD Deficiency | X-linked disorder, oxidative stress causes RBC hemolysis | Unconjugated | 1st week | Jaundice with triggers (fava beans, infections, drugs) | Avoid triggers, phototherapy, transfusion if severe |
| Hereditary Spherocytosis | Defect in RBC membrane proteins (ankyrin, spectrin) | Unconjugated | Early onset | Spherocytes on blood smear, splenomegaly, Coombs negative | Phototherapy, splenectomy later in life |
| Cephalohematoma / Birth Trauma | Extravasation of blood from birth trauma | Unconjugated | 2–3 days | Bruising, cephalohematoma, prolonged jaundice | Phototherapy if needed, resolves spontaneously |
| Breastfeeding Jaundice | Insufficient milk intake → dehydration | Unconjugated | First week | Dehydration, weight loss | Increase feeding frequency, lactation support |
| Breast Milk Jaundice | Inhibitory substances in breast milk delay bilirubin metabolism | Unconjugated | 1–2 weeks | Well-appearing baby, prolonged jaundice | Temporary formula feeding if levels are very high |
| Neonatal Sepsis | Infection (bacterial, viral) leading to liver dysfunction | Mixed (Unconj. & Conj.) | Variable | Poor feeding, lethargy, temperature instability | IV antibiotics, supportive care |
| Congenital Hypothyroidism | Defective bilirubin metabolism due to thyroid hormone deficiency | Unconjugated | Prolonged (>2 weeks) | Hypotonia, large fontanelle, constipation | Thyroid hormone replacement |
| Biliary Atresia | Obstruction of bile ducts → impaired bile flow | Conjugated | >2 weeks | Pale stools, dark urine, hepatomegaly | Surgical intervention (Kasai procedure) |